Marketplace Pulse: Medicaid and Marketplace Provider Networks
The Marketplace Pulse series provides expert insights on timely policy topics related to the health insurance marketplaces. The series, authored by RWJF Senior Policy Adviser Katherine Hempstead, analyzes changes in the individual market; shifting carrier trends; nationwide insurance data; and more to help states, researchers, and policymakers better understand the pulse of the marketplace.
Access to a network of providers is one of the most fundamental benefits of health insurance. Especially in highly regulated markets such as Medicare Advantage and the Affordable Care Act Marketplace, plans that are relatively standardized in terms of covered benefits and actuarial value may differ primarily by the nature of their provider networks. Plans use provider networks for brand differentiation. They also use networks to control costs, either by contracting with less expensive providers or by curtailing utilization with a narrow network that creates friction through wait times and long distances. Plans are incentivized to make their networks look as extensive as possible, sometimes resulting in directories populated by providers who are not actually willing to provide services. For consumers, provider networks have historically been a pain point, due to problems with both accuracy and adequacy. Federal and state regulators continue to wrestle with appropriate responses that navigate the tradeoff between access and cost.
In the context of the imminent unwinding of the Public Health Emergency and the associated redetermination of millions of Medicaid enrollees, interest in provider networks is heightened, because many consumers are expected to transition from Medicaid to Marketplace coverage. To minimize disruption in care, maintaining continuity of providers is a priority. Since many insurers participate in both markets, there is a general expectation that consumers will be steered to the Marketplace plans offered by their Medicaid insurers. Given this transition, it is important to understand both the differences between provider networks in Medicaid and the Marketplace, and also the degree of overlap in networks for insurers that have plans in both markets.
To improve understanding of this issue and to foster analysis of provider networks, the Robert Wood Johnson Foundation, in partnership with Ideon, has released network data for Medicaid and Marketplace plans. This release is designed to allow researchers, advocates, journalists, and policymakers to assess the status of provider networks in these markets. These data are obtained directly from insurers, and therefore contain many of the inaccuracies found in provider directories. A public resource allows high level comparisons, and licenses to more granular data are available at no cost for non-commercial use. These data are designed to permit the comparison of network characteristics by plan, specialty, specific geographies, and market segment. A recent webinar described the data and how it can be used. Additional information can be found here.
In general, these data show that Marketplace plans have larger networks. The overlap in provider networks between Medicaid and Marketplace is often small, meaning that even though consumers may be migrating to a plan where there are more choices, there is a high likelihood that they will be required to find a new provider. Preliminary analysis suggests that insurers who specialize in Medicaid generally have smaller Marketplace networks, but more overlap between their Medicaid and Marketplace networks. In fact, some plans have a nearly complete overlap between the two markets. Other insurers have relatively large networks in both their Medicaid and Marketplace plans, but very little overlap between the two. These patterns vary significantly by insurer, region, and specialty.
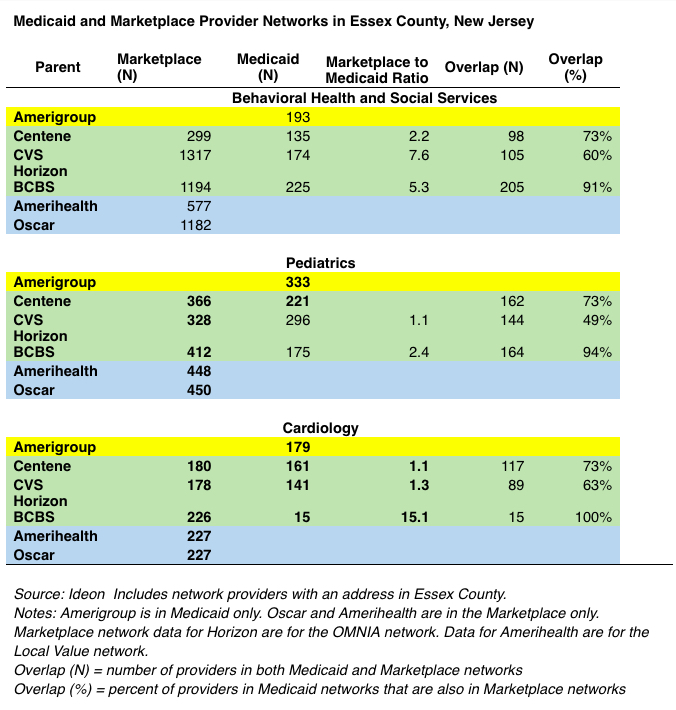
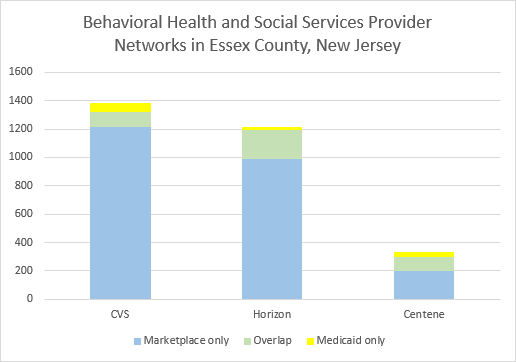
Essex County, New Jersey, provides an example of what this looks like in a particular place. There are five insurers in Essex County offering Marketplace plans, and four offering Medicaid plans. Three parent carriers offer plans in both markets. We can use the examples of behavioral health, pediatrics, and cardiology to see how these networks compare. Networks include providers listing addresses in Essex County. Looking first at Marketplace plans, the behavioral health specialty has the biggest range in network size. Horizon, CVS, and Oscar report much larger Marketplace networks than does Amerihealth or Centene. For the other two specialties, Centene and CVS have smaller networks compared to Horizon, Oscar, and Amerihealth, but the difference is not as great. For all three specialties, Medicaid networks are smaller than Marketplace networks, with the greatest difference between the two in the behavioral health specialty. An important caveat about behavioral health services in New Jersey is that the state "carves out" some aspects of that specialty, meaning that the networks reported by these insurers don't necessarily represent to full extent of services available to Medicaid enrollees. For pediatrics and cardiology, the difference between Medicaid and Marketplace networks is generally smaller, although Horizon has reported an extremely small number of cardiologists in their Medicaid network.
From this limited example, it would appear that Medicaid enrollees in Essex County who transition to the Marketplace plan offered by their Medicaid carrier have a reasonable chance of keeping their providers, at least for these specialties. For example, Horizon reports more than 90% overlap in all three specialties, meaning that at least 90% of the providers in their Medicaid network are also in their Marketplace network. For Centene, the overlap rate is 73% for all three specialties, and for CVS the overlap ranges between 49% and 63%. Provider overlap varies considerably by region, specialty, and insurer, and is an important consumer issue in the context of Medicaid redetermination.
Another takeaway from this example is that Medicaid networks appear to be considerably smaller than Marketplace networks, even though the size of the Medicaid population is far greater.
New Jersey had about 311,000 Marketplace enrollees in 2023, versus approximately 2.2 million enrolled in Medicaid. Essex County alone has about 250,000 Medicaid enrollees. County-level Marketplace enrollment information for New Jersey in 2023 is not available, but Essex County is unlikely to have more than 40,000 Marketplace enrollees. Therefore, Marketplace networks in Essex County appear to be much larger, even though they serve far fewer people. This suggests there may be a notable gap in access to care between Medicaid and Marketplace enrollees. That pattern is consistent with findings from a 2021 study, which showed that emergency department use was higher and office visit rates were lower among Medicaid versus Marketplace enrollees in Colorado, suggesting that smaller Medicaid provider networks may have curtailed utilization. This may also be the case in New Jersey, since Medicaid provider networks appear to be far smaller. The impact on health outcomes from such a gap is not known, but there are clearly equity, cost, and quality implications.
Due to the well-known inaccuracies in provider directories, it may be the case that these access differences are smaller or larger than they appear. Providers listed in directories often are not willing to provide services to enrollees that attempt to contact them, either because they don’t actually participate in the network or because they are only willing to participate in a very limited fashion. If the providers listed in the Medicaid networks are more intensively engaged in providing services than are the providers listed in the Marketplace networks, then the differences in network size may overstate the difference in access. If the reverse is true, then the gap in access may be even greater than it appears. One of the reasons for releasing these data is to improve understanding of the true nature of provider access in Medicaid and Marketplace plans to better inform policy discussions about access, cost, and quality of care. We hope these data will be used to answer these important questions.
Related Content

Marketplace Pulse
