Marketplace Pulse: What's Going on With Medicaid Redetermination?
The Marketplace Pulse series provides expert insights on timely policy topics related to the health insurance marketplaces. The series, authored by RWJF Senior Policy Adviser Katherine Hempstead, analyzes changes in the individual market; shifting carrier trends; nationwide insurance data; and more to help states, researchers, and policymakers better understand the pulse of the marketplace.
This piece is co-authored by Wyatt Bensken, PhD, research investigator, OCHIN, Inc.
The Medicaid redetermination process is largely complete, but we are only beginning to understand the impact on enrollees and providers. Data on pediatric encounters from a large network of Community Health Centers (CHCs) provides an early perspective on how coverage and payer mix is changing. Highlights include a decline in the overall volume of Medicaid-insured visits and an increase in the share of visits from uninsured patients, with little variation among states.
During the federal COVID-19 Public Health Emergency (PHE), and formalized in subsequent legislation, the federal government incentivized states to keep people enrolled in the Medicaid program. In exchange for additional federal Medicaid funding, states were prohibited from conducting routine eligibility redeterminations. Enrollment in Medicaid increased by approximately 20 million nationally during the three-year “continuous coverage” period. However, beginning April 1, 2023, states were required to resume eligibility determinations and complete the process within a 12-month period (“unwinding”).
Not surprisingly, redetermination is predicted to cause significant changes in coverage status. About 15 million enrollees are expected to lose their eligibility for Medicaid. While all would ostensibly be eligible for an affordable offer of coverage through employers or the individual market, not all offers will be taken, with the result that approximately 3 million people are estimated to become uninsured. Redetermination is also an administrative undertaking with no real precedent, as three years of annual eligibility reviews are compressed into a one-year period, in a context where many enrollees and Medicaid staff lack recent experience with the process. In addition to projected coverage changes resulting from loss of Medicaid eligibility, it is also expected that some coverage loss, despite eligibility, is expected to occur as a byproduct of the process.
One issue that has captured a lot of attention is the extent to which states have struggled to accurately conduct their eligibility redeterminations, and the number of enrollees who have lost their Medicaid coverage because of a “procedural termination”—that is that an individual did not complete the renewal process. Of the estimated 16.4 million people who have lost their Medicaid coverage during the first ten months of redetermination, approximately 70% had their coverage terminated for procedural reasons. While this may mean that enrollees have already moved on to other coverage, it more often reflects poor communication between state agencies and enrollees, resulting in the inadvertent termination of enrollees who remain eligible. While enrollees who erroneously lose coverage should be able to successfully reenroll, it is not clear that all will do so and how long that process will take.
Therefore, the longer-term coverage impact of redetermination is unclear, since it’s too soon to know how much of the current disenrollment reflects actual eligibility loss, how many of those who are procedurally terminated will successfully reenroll in Medicaid, and how many of those who lose Medicaid eligibility will migrate to other coverage versus becoming uninsured. If overall coverage loss is significant and sustained, the impact on patients and providers is clearly major, as care is interrupted for patients and providers lose an important source of revenue. Concerns about these potential effects are heightened since almost four million of those who have lost coverage are children.
Even if coverage patterns generally return to pre-pandemic baseline, redetermination represents a significant change for Community Health Centers (CHCs) that care for many patients with Medicaid. CHCs are the frontline primary care organizations that serve America’s systemically marginalized patients, providing care for over 30 million people in the United States, including one in nine children.
However, despite federal funding, CHCs have narrow financial margins and are particularly exposed to the impact of the unwinding of continuous Medicaid coverage. An increase in uninsured patients coupled with a decrease in Medicaid reimbursements is already creating a strain, as detailed in a recent New York Times article that described interruptions in children’s care, financial stress for parents, and serious revenue problems for clinics in Texas.
In this context, timely data from CHCs offers a useful window into current trends. We used data from the OCHIN national network of CHCs to examine changes in encounter-level payer mix before the PHE, during continuous coverage, and during unwinding. This analysis is based on more than 4.5 million visits from pediatric patients at 1,325 clinics from 85 different organizations between January 1, 2019, and December 31, 2023. Of note, the populations that OCHIN members serve mirrors that of all CHC patients nationwide.
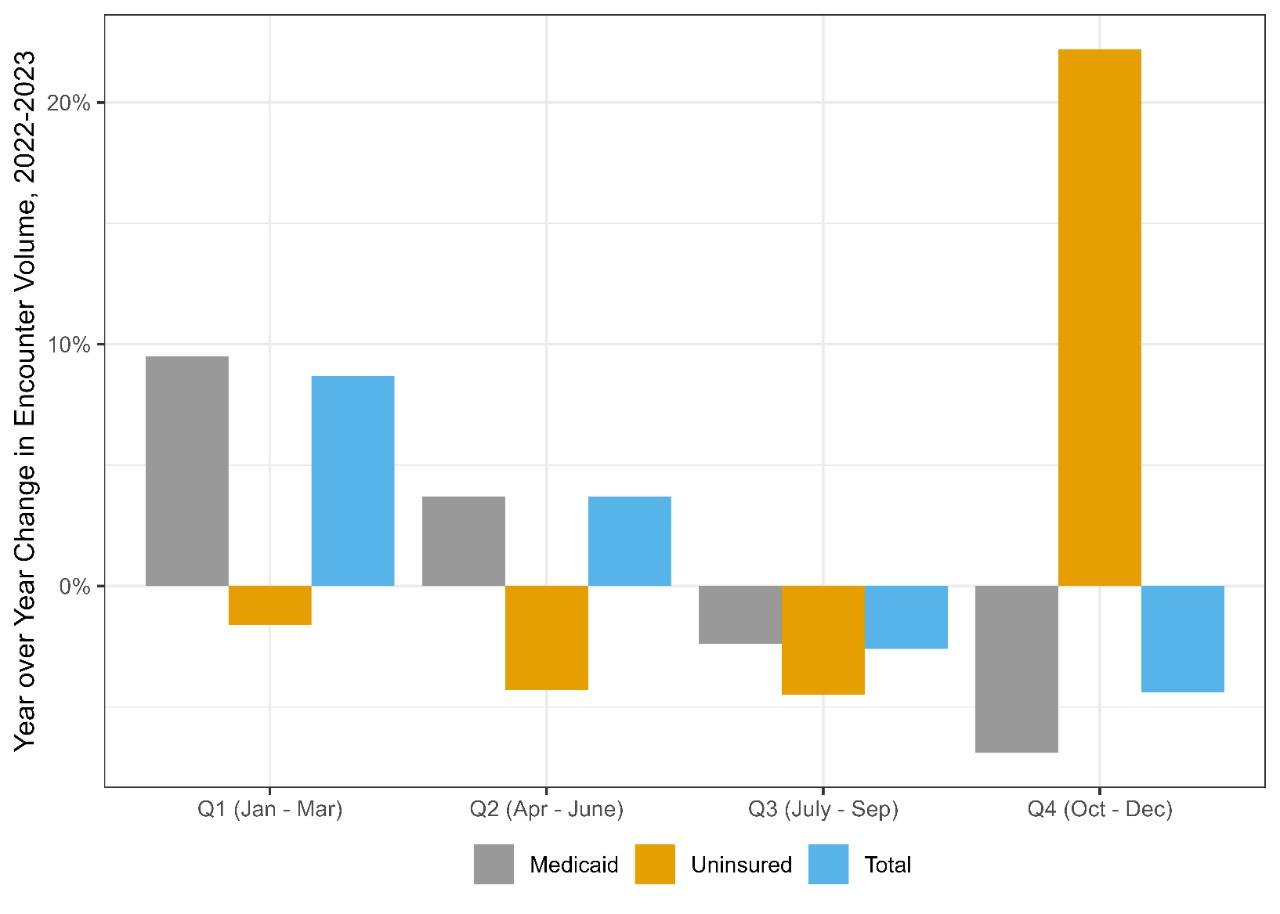
There are several main takeaways. As expected, overall visit volume declines, driven by a reduction in Medicaid encounters. The changes are not dramatic but appear to accelerate in later months of 2023. So, while Medicaid visits in the third quarter (Q3) 2023 were only 2.5% lower than in Q3 2022, by Q4 2023 the number of Medicaid-insured encounters was 7% lower than the year before. This trend may worsen as more states complete the redetermination process, though it could also be moderated as people who are procedurally terminated become reenrolled. Additionally, there are some countervailing trends that would be expected to increase Medicaid visits, since several states have recently added postpartum eligibility.
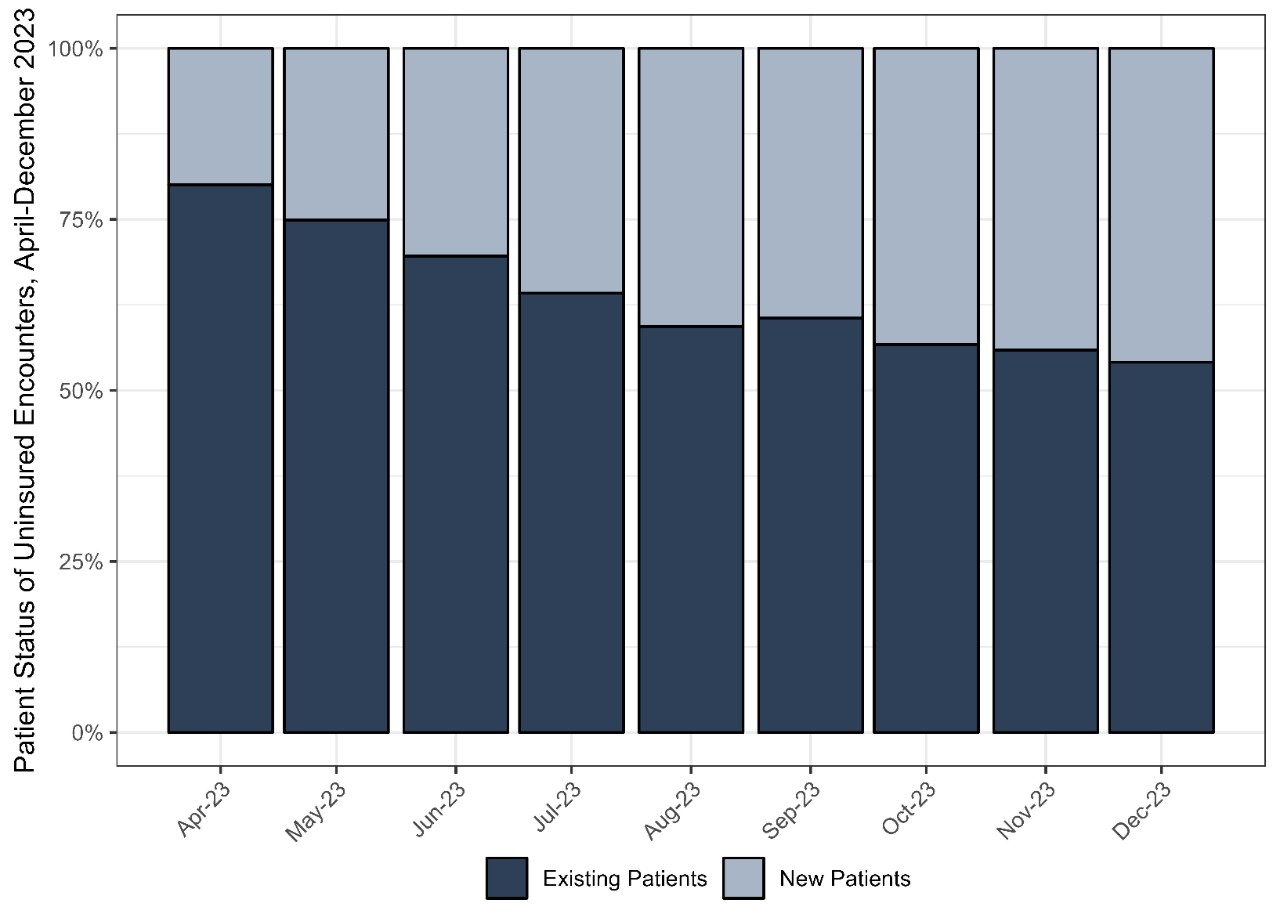
Relatedly, the proportion of visits from uninsured patients began to increase, exceeding 12% of all visits in the last two months of 2023. The number of visits from uninsured patients increased somewhat as well, with a year over year increase of 22.2% in Q4 of 2023. As the unwinding period progressed, the share of uninsured encounters that were new patients (defined as patients that had not had a visit between March 2021 and March 30, 2023) increased, growing from 19.9% to 45.9% between April and December 2023. The share of new patients that were uninsured similarly increased over time, from 16% to 18%, suggesting that some patients who had been receiving care elsewhere may have visited a CHC after losing their Medicaid coverage. Despite notable differences between states in the timing of and approach to redetermination, these broad patterns varied little among the states where OCHIN members were well-represented (Calif., Ind., Mass., Minn., Mont., N.C., Ohio, Ore., Texas, and Wash.).
So far, redetermination has led to modest but discernible changes in volume and payer mix in CHCs reflecting coverage loss associated with redetermination. Additional data will show whether these trends continue or worsen and can provide more information about types of visits and whether similar patterns are observed among adults. A limitation is that CHCs have a narrow market share, but importantly, they serve a disproportionate share of patients without insurance. Supplementing these data with encounter data from statewide sources such as all-payer claims databases or acute care data can help paint a fuller picture of how redetermination may affect access to other types of care at the population level. Despite these limitations, these data show that redetermination so far is affecting access to care for low-income children and revenue for providers that serve them.
Additional results can be found in the corresponding Research Data Brief from OCHIN at https://advancecollaborative.org/medicaid-policy-impact-marginalized-populations. This work was funded by the Robert Wood Johnson Foundation.
Related Content

Marketplace Pulse Library
